What is shoulder impingement syndrome?

Shoulder impingement syndrome is when there is reduced clearance between the humeral tuberosities and the coracoacromial arch during elevation, which pinches the intervening soft tissues. The vulnerable soft tissues are the subacromial or subdeltoid bursa, the rotator cuff tendons and the long head of biceps. (CSP guidelines)
Classification:
Primary
Secondary
Internal Glenoid Impingement
Anatomy of the shoulder:
Before we discuss the above classifications further, you need to know a bit about the anatomy of the shoulder:
Bone:
Scapula:

Clavicle:

Humerus:

Joints:
Glenohumeral joint:
Scapula (glenoid) and humerus
Sheroidal
Shallow glenoid
Large head of humerus
Labrum around glenoid
Closed packed position: full abduction and external rotation
Capsular pattern: ER >ABD>IR>Flex
Very mobile and unstable
Sternoclavicular joint:
Sternum to clavicle
Saddle joint
Closed packed position: Arm abducted to 90
Acromioclavicular joint:
Clavicle to scapula (acromion)
Plane synovial
Closed packed position: Arm abducted to 90
Scapulothoracic joint:
Underside of scapula with thorax (ribs)
No true articulation
Main muscles of the shoulder (excluding the rotator cuff):
Trapezius:

Levator Scapulae:

Rhomboids:

Latissimus Dorsi:

Serratus anterior:

Deltoid:

Pectoralis Major:

Pectoralis Minor:

Biceps Brachii:

Triceps Brachii:

Muscles of the rotator cuff:
Supraspinatus:

Supraspinous fossa of scapula to greater tubercle of humerus
Assists deltoid in abd of humerus
Infraspinatus:

Infraspinous fossa of scapula to greater tubercle of humerus
Externally rotates the humerus
Teres Minor:

Lateral border of the scapula to Greater tubercle of humerus
Externally rotates the humerus
Subscapularis:

Subscapular fossa of the scapula to lesser tubercle of humerus
Internally rotates the humerus
Teres Major:

(Technically not part of the rotator cuff) Inferior angle of scapula to intertubercular groove of humerus
Internally rotates and adducts the humerus
Labrum:

Soft fibrous tissue rim called the labrum surrounds the socket to help stabilize the joint. The rim deepens the socket by up to 50% so that the head of the humerus fits better. In addition, it serves as an attachment site for several ligaments
Bursae:

Fluid filled sacs that help to reduce friction. The sub-acromial bursa is the most commonly inflamed of the shoulder bursae
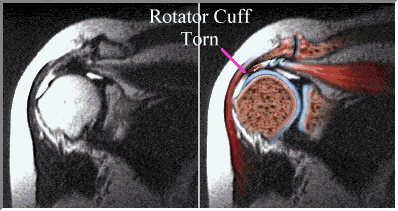
Primary impingement or external-Subacromial impingement:
An area of the Rotator cuff is torn or irritated. Typically the superior or bursal side is the area affected. This means the source of pathology is outside of the glenohumeral joint itself and confined to the Subacromial space, hence usage of the word ‘external’. (Andrews, 1994).
Primary SIS typically affects people older than 50 years of age although it can happen in the young but it is less likely.
Pain is often felt in the anterior or front of the shoulder during overhand activities. They can get pain at night when they roll onto that shoulder.
Causes of primary SIS:
Consequence of the aging process
Mechanical compromise of the subacromial space
Degenerative Joint Disease of the acromioclavicular (A/C) joint
Subacromial spurring
Rotator cuff atrophy
Rotator cuff/scapular weakness
Increased thoracic kyphosis
Poor posture
Diagnosis of primary SIS:
Due to the degenerative nature of primary SIS an X-ray is useful. Here you can analyse the shape of the acromion process of the scapula (shoulder blade) as this plays a big part in recovery.

Type I: Flat acromion low incidence of impingement
Type II: Curved acromion higher incidence of impingement
Type III: Beaked acromion very high incidence of impingement
Type III is usually genetic but it may be a previous Type II that has degenerated into a type III.
95% accuracy with Hawkins-Kennedy, painful arc and infraspinatus muscle test grouped together

Prognosis of primary SIS:
Types I and II usually recover with conservative care, which will take at least 6 months to rehabilitate. Scapular control and coupled rotator cuff activation is vital to normal shoulder function (Kilber et al 2001). Muscles around the shoulder function in an integrated fashion and should be rehabilitated in integrated patterns (Kilber et al 2001).
Closed chain axial loading exercises are the primary means of early shoulder rehab & functional rehab protocols (Kilber et al 2001).
Functional shoulder rehab: Activations & joint motions follow a proximal-to-distal pathway along the kinetic chain (Kilber et al 2001).

Congenital type III’s may recover without surgery but often need it. Degenerative type III’s will require surgical debridement before the spur causes a rotator cuff tear. If a tear occurs then it will need to be repaired and these types of patients do not do as well.
Secondary Impingement:
This is when there is a problem with keeping the humeral head centred in the glenoid fossa during movement of the arm. Generally this is caused by functional instability (neuromuscular control) combined with a laxity in the glenohumeral joint capsule and ligaments.
Secondary impingement generally occurs in the coracoacromial space due to anterior translation of the humeral head as opposed to the Subacromial space that is seen in primary impingement.
Patients are usually younger and pain is commonly felt in the anterior or anterolateral aspect of the shoulder. The symptoms are usually activity specific and involve overhand activities.
Causes of secondary impingement:
Rotator cuff weakness
Functional instability
Congenital Capsular laxity
Acquired capsular laxity from trauma (e.g. dislocation)

Diagnosis of secondary impingement:
There is insufficient evidence upon which to base selection of physical tests for shoulder impingements (Hanchard et al 2013)
For secondary impingement it is important to look at the history (e.g. previous trauma, hypermobility syndrome etc.)
Testing should examine the passive and active stability of the joint.

Prognosis of secondary impingement:
Exercise works!!!!
It will take at least 6 months of rehabilitation. Scapular control and coupled rotator cuff activation is vital to normal shoulder function (Kilber et al 2001). Muscles around the shoulder function in an integrated fashion and should be rehabilitated in integrated patterns (Kilber et al 2001).
Closed chain axial loading exercises are the primary means of early shoulder rehab & functional rehab protocols (Kilber et al 2001).
Functional shoulder rehab: Activations & joint motions follow a proximal-to-distal pathway along the kinetic chain (Kilber et al 2001).
What about an injection?
Accuracy with the needle is between 37-70%, which obviously lessens the chance of it working.
What actually causes the effect? Is it the steroid or is it the anaesthetic or even the needle itself?
The other issue with injection is that it has deleterious effects and so will weaken the tendon further
Evidence suggests short term efficacy only.
It is most effective at 1 to 2 weeks from when the injury started possibly due to higher levels of inflammation?
Internal Glenoid Impingement, also called posterior-superior glenoid impingement (PSGI):

This is probably the most common cause of posterior shoulder pain.
It is commonly misdiagnosed as rotator cuff tendinopathy. (Jobe, 1995)
PSGI is caused by the impingement of the posterior edge of the supraspinatus and the anterior edge of the infraspinatus against the posterior-superior-glenoid and glenoid labrum.
It is commonly seen in overhead athletes and patients involved in occupational overhead activities.
The mechanism of injury is shoulder extension, abduction and ER mechanism. This is the exact mechanism the arm is in when you try and throw a ball overhand. (Arroyo, 1997)
Causes of PSGI Instability as a cause of PSGI:
Chronic repetitive eccentric loads on the subscapularis from throwing lead to micro-trauma and weakness. Loss of the subscapularis force couple leads to anterior instability.
Scapular Dyskinesia (abnormal shoulder blade motion)
Diagnosis of internal glenoid impingement:
Done through the symptom history and patient presentation:
Posterior shoulder pain in the throwing shoulder
Slow insidious onset with no history of trauma
Pain is primarily associated with the athletic or work activity
Prognosis of internal glenoid impingement:
Avoidance of aggravating activities
Strengthening of the rotator cuff muscles
Scapular setting exercises and functional rehab as in previous impingement types
If rehabilitation is not successful then surgery can be performed:
Anterior capsulo-labral reconstruction
Thermal Capsulorraphy (TACS-Thermal Assisted Capsular Shrinkage)
(Jobe 1997)
Summary of SIS:
How common is SIS overall?
74% of patients in primary care are SIS.
Rehabilitation exercises are always needed and the exercise effect is even better with manual therapy.
Комментариев нет:
Отправить комментарий