Не знаем, поможет ли продолжение статьи развеять мифы или только подольет масла в огонь про слабое женское “дно”, но призываю вас очень внимательно ее прочесть. Есть над чем задуматься, потому что я попала как раз в те 93% женского населения, которое ничего об этом не знает.
Татьяне вежливо и не очень указывали, что она ничего не понимает в женских тренировках; одобряет тех, кто толстеет на диване; запугивает почем зря спортивных девушек, хотя никакого вреда для здоровья женщин в грамотной работе с весом нет…
Поэтому Татьяна написала продолжение
«Чтобы не казалось, что я всё выдумываю относительно тяжестей и дисфункции тазового дна у женщин, я снабдила текст ссылками на PubMed — это одна из самых больших в мире баз данных медицинских исследований.
Не уверена, что это защитит меня от дальнейших нападок, но здравомыслящим людям будет интересно.
ПРО ЖЕНСКИЕ ТРЕНИРОВКИ
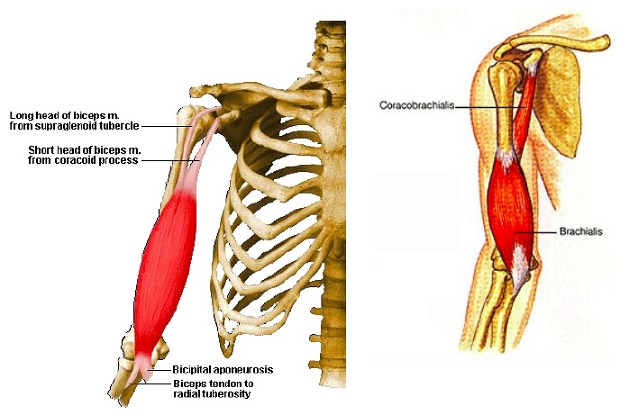
Выражение «слабый пол» появилось не потому, что женщина не способна носить тяжести, а в связи с тем, какие за этим следуют проблемы. Только с точки зрения анатомии нас правильнее было бы называть не слабый пол, а «слабое дно». Тазовое дно. У женщин в тазовой диафрагме есть расширение вокруг шейки матки (см.иллюстрацию). То есть мочевой пузырь, матка, яичники НЕ имеют мышечной поддержки снизу. В то время как у мужчин там плотное соединение мышц с фасцией, что логично: шейки матки и продолжения в виде влагалища у них нет.
За то, чтобы органы находились на своих местах и нормально функционировали, отвечает не только этот мышечный гамак, но и связки. С их помощью матка, трубы, яичники и прочий ассортимент крепятся к костям таза.
Чтобы понять разницу между свойствами мышц и связок, представьте себе надувной шарик и полиэтиленовый пакет: один эластичный, может растягиваться и сокращаться, другой — только растягиваться.
Поэтому стоит иметь в виду, что упражнения Кегеля и другие системы укрепления интимных мышц воздействуют именно на мышцы. Связкам они не способны вернуть первоначальную длину и силу.
Как только вышеуказанная поддерживающая конструкция теряет свою упругость, начинается процесс опущения внутренних органов, или пролапс.
Это вообще не смертельно и даже не болезнь, но способно отравить жизнь. Возникают боли в нижней части спины, ноет живот или там появляется чувство тяжести; сложнее достичь оргазма, более того — женщины могут испытывать боль во время секса.
Кстати, попадающий во влагалище воздух в процессе близости или упражнений — один из признаков начавшегося ослабления мышц тазового дна (если это происходит не только во время овуляции, но и на протяжении всего цикла). Нарушается цикл, возникают сложности с тем, чтобы забеременеть…
Постепенно из-за смещенных органов начинается недержание мочи, стоит только чихнуть или покашлять. Еще из неприятностей — газы в кишечнике и вероятность не удержать это в себе не в самый подходящий момент. И наоборот, мучают запоры… Потом что-то настойчиво мешается во влагалище, а на последних стадиях пролапса влагалище и вовсе выпадает полностью.
Кстати, говорить об этом не принято. По одной из ссылок, указанных ниже, можно найти статью, в которой признается, что женское здоровье, весь этот дискомфорт — это «культура замалчивания»…
Почему происходит опущение? Я думаю, все началось, когда человек в ходе эволюции встал на две ноги. Млекопитающие ходят на четырех конечностях, и нагрузка на тазовое дно у них распределяется иначе, чем у homo sapiens.
В медицинской же литературе называются следующие факторы:
-врожденная дисплазия соединительной ткани. Под подозрение попадают люди с растяжками на коже, варикозным расширением вен, склонностью к образованию синяков, диастазом прямой мышцы живота, а также пупочной грыжей, гипермобильностью суставов.
-пол. Из анатомической справки выше нам известно, что у женщин тазовая диафрагма ослаблена в передней части. Поэтому процент пролапса у нас выше, чем у мужчин.
-беременность и роды. Это опять про женщин и тут чистая физика: одно дело держать маленькую матку, совсем другое — к девятому месяцу справляться с весом малыша, околоплодных вод, плаценты… В родах, чтобы шейка матки открылась, мышцы должны растянуться еще сильнее.
-ожирение. Лишний вес — это не только жир под кожей, но и вокруг внутренних органов, так называемый висцеральный. Это тоже лишняя тяжесть для тазового дна, и хотя бы поэтому важно следить за весом.
-малоподвижный образ жизни. Тканям не хватает питания, и они ослабевают.
-эстрогенная недостаточность. Возникает, например, в результате «бешеной сушки» или в период менопаузы. Без достаточного количества эстрогенов ткани нашего тела теряют эластичность. По данным различных исследований, в пожилом возрасте частота пролапса гениталий у женщин возникает в 50-75% случаев.
-систематическое повышение внутрибрюшного давления. Причиной его может быть и хронический запор, и кашель в результате бронхита или астмы, и регулярный физический стресс от тяжелой работы, и подъем тяжестей.
Про внутрибрюшное давление подробнее.
Мы так устроены, что неважно, взваливаем на себя мешок в картошкой или делаем становую тягу, — оно повышается. Систематическая работа с большим весом медленно, но верно выдавливает мышцы тазового дна и растягивает связки, на которых крепятся органы.
Ношение подрастающих детей на руках тоже создает риски пролапса. В исследовании «The effects of walking speeds and carrying techniques on intra-abdominal pressure in women» (Coleman TJ,Hamad NM,Shaw JM,Egger и прочие) женщинам внутривагинально устанавливались датчики. Приборы зафиксировали, что скорость ходьбы и ношение малыша на руках вносит значительные изменения во внутрибрюшное давление.
Только не спрашивайте меня «И что же, теперь не поднимать детей?» — это не ко мне вопрос, а к Творцу: он поставил нас на две ноги, выдал нам слабую диафрагму, организовал роды и детей, которых мы, в отличие от млекопитающих, носим на руках, — где справедливость?
И есть ли безопасный для женского здоровья вес?
Я задала этот вопрос американскому физиотерапевту Линн Шульте, которая занимается в том числе реабилитацией тазового дна после родов. По её мнению, в идеале женщине достаточно работать с собственным весом, избегая гантелей и штанги вообще.
Автора другой версии, про то, что это не более 5 кг (+/- , в зависимости от индивидуальных особенностей женщины), не подскажу, выяснить не удалось. Но этот взгляд основан на том, что мышцы тазового дна способны выдержать во время беременности вес растущего ребенка, околоплодных вод, плаценты, то есть в районе 5 кг.
Данные одного из исследований говорят, что существенное влияние на состояние мышц тазового дна оказывает вес от 10 кг:
http://www.ncbi.nlm.nih.gov/pubmed/19384125А в другом анализе у женщин детородного возраста, чья работа связана с ношением тяжестей от 20 кг, обнаружено опущение шейки матки по сравнению с контрольной группой легкой нагрузки.
«Расшатывают» тазовое дно у женщин не только тяжести и качание пресса, но и виды физической нагрузки, где приходится бегать и прыгать. Так называемая высокая отдача упоминается в статье
link.springer.com/article/10.2165/00007256-200434070-.. , посвященной молодым нерожавшим спортсменкам. Согласно статистике, в зависимости от вида нагрузки — баскетбол, легкая атлетика и т.д., девушки страдают в той или иной степени недержанием мочи. Причем, у тех, кто играет в гольф, такой проблемы нет вообще, а вот у тех, кто занимается прыжками на батуте, она зашкаливает — до 80%.
Эта информация раздражает: вдруг выяснить, что собственноручно прокладываешь тропинку для дисфункция _тазового_дна, когда думала, что ведешь здоровый_образ_жизни и вызываешь восхищение спортивными формами… В качестве защитной реакции мне приводят в пример знакомых девушек, которые работают в зале с весом, и у них все в порядке. Верю! Только опущение внутренних органов — не моментальный процесс, вероятность и скорость его появления зависит от сочетания нескольких факторов: генетическая прочность соединительной ткани, количество беременностей, родов и травм в них, нагрузка, которая приходится на организм…
Моментом истины станет менопауза, когда ресурсы нашего тела уменьшаются. В одном из многочисленных исследований проблемы (
http://www.ncbi.nlm.nih.gov/pubmed/20607975) упоминается, что распространенность опущения женских органов в будущем будет еще выше в связи с увеличением продолжительности жизни женщин.
Что делать с этой информацией — каждая из нас решит для себя сама. Когда на одной чаше весов современные стандарты красоты, на другой — женское_здоровье и комфортная старость, важно сделать информированный выбор.
Кстати, про это тоже есть исследования: молодых нерожавших женщин попросили оценить их знания относительно тазового дна. В общей сложности 93% женщин оказались не в курсе устройства собственного тела и рисков развития пролапса гениталий (
https://www.ncbi.nlm.nih.gov/m/pubmed/27313364/?i=1.. ). Поэтому в наших интересах не брезговать информацией.





 Присед со штангой над головой
Присед со штангой над головой