Pelvic, Trunk, and Scapula stability need to be secure to prevent common rotator cuff injuries
A survey of one year (2006) showed that over 7.5 million people visited their doctor for a shoulder problem, including shoulder and upper arm sprains and strains. More than half of these visits (4.1 million) were for rotator cuff problems. Another more recent study (Lewis, 2014) reported that 70% of visits to doctors and therapists for shoulder pain were related to rotator cuff disorders.
Shoulder injuries are frequently caused by sports and athletic activities that involve excessive, repetitive, overhead motion, such as swimming, racket sports, throwing, and weight-lifting. However, many of these injuries occur during everyday household and occupational activities such gardening, cleaning, and painting.

Subscapularis is located on the anterior surface of the scapula between the scapula and the ribs and attaches to the humerus.
Anatomy
The group of muscles collectively known as the rotator cuff controls the motion of the head of humerus, the “ball” in the ball and socket joint of the shoulder (glenohumeral joint). The “socket” part of the joint is the glenoid fossa of the scapula, so as the scapula moves so does the socket. The rotator cuff muscles act to keep the ball of the shoulder joint secured in the right position in the socket.
The rotator cuff group comprises supraspinatus, infraspinatus, teres minor and subscapularis. Each of these muscles has a unique primary action, but they also act together as a stabilising unit. When used for primary action, subscapularis acts as an internal rotator, infraspinatus and teres minor as external rotators, and supraspinatus as an arm abductor.
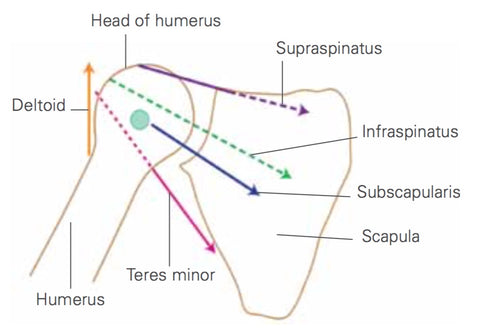
Directions of pull of the rotator cuff muscles
Movement and Stability
As stabilisers, these muscles exert a compressive force on the head of humerus to secure it in the socket during arm movements. In effect they suck the head of the humerus into the socket, providing a stable axis for arm movement. Without the rotator cuff’s stabilising action, the more superficial movement muscles pull the head of humerus across the socket as they contract. The fixed point, or movement axis, is lost and the muscular pattern for force production and shoulder control altered. If the head of humerus is allowed to slide up or forward in the socket, it can press against bony and ligamentous structures in the shoulder, causing tissue trauma and painful pathologies such as tendonitis and instability.

Correct and efficient rotation of the shoulder around its axis requires pelvis, trunk, and scapula stability
Trigger Points
Trigger points, insofar as we accept them as part of the body's natural protect and defense mechanism, are often a good indicator of postural and stability issues. Early identification and treatment is therefore always likely to be beneficial.
Trigger points make their host muscles shorter and weaker and trigger points in the rotator cuff muscles left untreated may lead to a number of painful shoulder disorders.
Injury Prevention
Rotator cuff training alone will not ensure shoulder health. Scapular stability is necessary to ensure that the socket is controlled and well positioned for whichever forces it must deal with. Trunk and pelvic stability is necessary to provide a supportive foundation for the scapula. If your trunk stability is poor, it is likely that your scapulae will be dragged into a poor position. Pelvic control problems can also alter scapular positioning, either directly due to excessive dependence upon latissimus dorsi, or indirectly by failing to provide a supportive platform for the trunk.
To protect the rotator cuff, make sure that your pelvic stability, trunk stability and scapular stability are secure in order to support good shoulder mechanics prior to performing resistance work for the upper body.
Ref: Stability, Sport and Performance Movement - Joanne Elphinstone
Комментариев нет:
Отправить комментарий