https://clinicalgate.com/shoulder-complex/
DONALD A. NEUMANN, PT, PhD, FAPTA
The study of the upper extremity begins with the shoulder complex, a set of four articulations involving the sternum, clavicle, ribs, scapula, and humerus (Figure 5-1). This series of joints provides extensive range of motion to the upper extremity, thereby increasing the ability to reach and manipulate objects. Trauma or disease often limits shoulder motion, causing a significant reduction in the effectiveness of the entire upper limb.
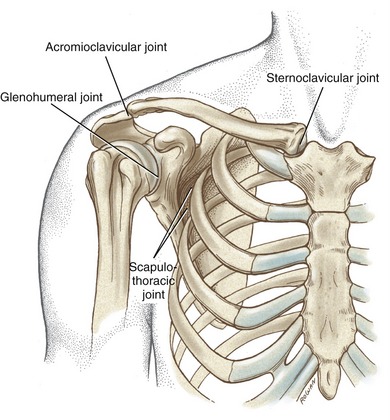
FIGURE 5-1. The joints of the right shoulder complex.
OSTEOLOGY
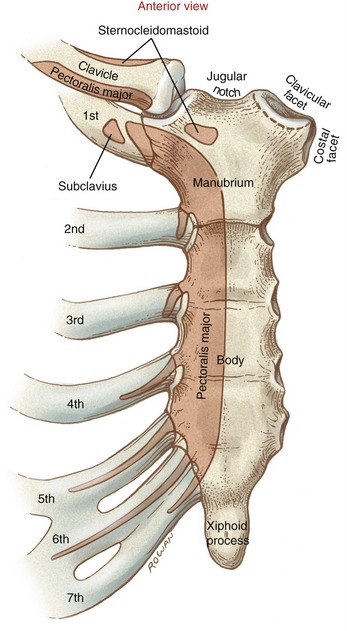
The sternum consists of the manubrium, body, and xiphoid process (Figure 5-2). The manubrium possesses a pair of oval-shaped clavicular facets,which articulate with the clavicles. The costal facets, located on the lateral edge of the manubrium, provide bilateral attachment sites for the first two ribs. The jugular notch is located at the superior aspect of the manubrium, between the clavicular facets.
Clavicle
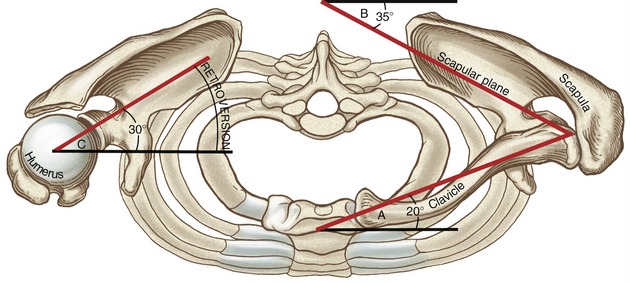
When one looks from above, it is evident that the shaft of the clavicle is curved, with its anterior surface being generally convex medially and concave laterally (Figure 5-3). With the arm in the anatomic position, the long axis of the clavicle is oriented slightly above the horizontal plane and about 20 degrees posterior to the frontal plane (Figure 5-4; angle A). The rounded and prominent medial or sternal end of the clavicle articulates with the sternum (see Figure 5-3). The costal facet of the clavicle (see Figure 5-3; inferior surface) rests against the first rib. Lateral and slightly posterior to the costal facet is the distinct costal tuberosity, an attachment for the costoclavicular ligament.
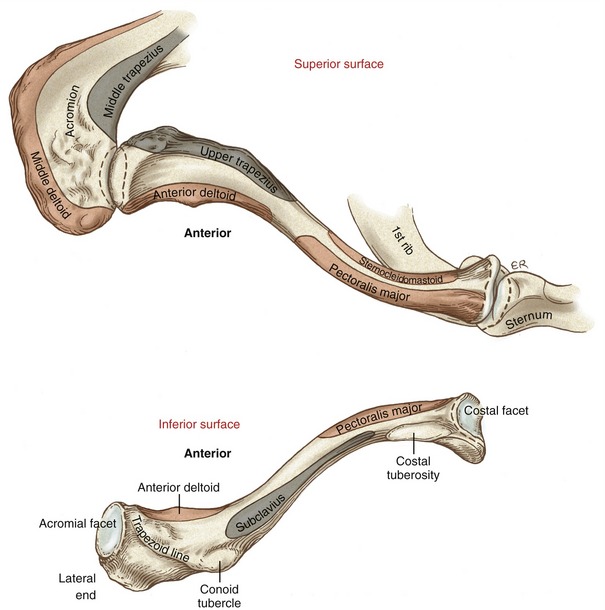
The lateral or acromial end of the clavicle articulates with the scapula at the oval-shaped acromial facet (see Figure 5-3; inferior surface). The inferior surface of the lateral end of the clavicle is well marked by the conoid tubercle and the trapezoid line.
Scapula
The triangular-shaped scapula has three angles: inferior, superior, and lateral (Figure 5-5). Palpation of the inferior angle provides a convenient method for following the movement of the scapula during arm motion. The scapula also has three borders. With the arm resting by the side, the medial or vertebral border runs almost parallel to the spinal column. The lateral or axillary border runs from the inferior angle to the lateral angle of the scapula. The superior border extends from the superior angle laterally toward the coracoid process.
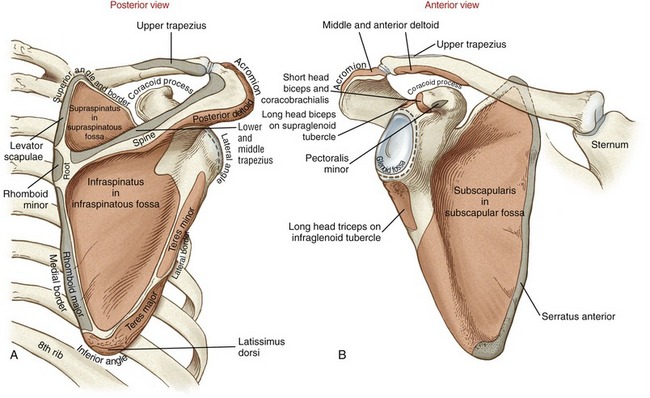
The posterior surface of the scapula is separated into a supraspinatous fossa and an infraspinatous fossa by the prominent spine. The depth of the supraspinatous fossa is filled by the supraspinatus muscle. The medial end of the spine diminishes in height at the root of the spine. In contrast, the lateral end of the spine gains considerable height and flattens into the broad and prominent acromion (from the Greek akros, meaning topmost, highest). The acromion extends in a lateral and anterior direction, forming a horizontal shelf over the glenoid fossa. The clavicular facet on the acromion forms part of the acromioclavicular joint (see Figure 5-16, B).
The scapula articulates with the head of the humerus at the slightly concave glenoid fossa (from the Greek root glene, socket of joint, + eidos,resembling) (see Figure 5-5, B). The slope of the glenoid fossa is inclined upward about 4 degrees relative to a horizontal axis through the body of the scapula.26 This inclination is highly variable, ranging from a downward inclination of 7 degrees to an upward inclination of nearly 16 degrees. At rest the scapula is normally positioned against the posterior-lateral surface of the thorax, with the glenoid fossa facing about 35 degrees anterior to the frontal plane (see Figure 5-4; angle B). This orientation of the scapula is referred to as the scapular plane. The scapula and humerus tend to follow this plane when the arm is naturally raised overhead.
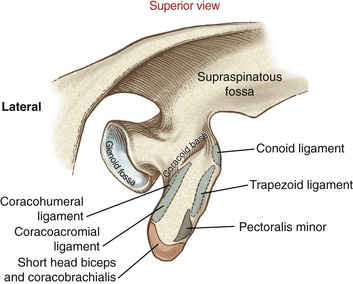
Located at the superior and inferior rim of the glenoid fossa are the supraglenoid and infraglenoid tubercles. These tubercles serve as the proximal attachment for the long head of the biceps and triceps brachii, respectively (see Figure 5-5, B). Near the superior rim of the glenoid fossa is the prominent coracoid process, meaning “the shape of a crow’s beak.” The coracoid process projects sharply from the scapula, providing multiple attachments for ligaments and muscles (Figure 5-6). The subscapular fossa is located on the anterior surface of the scapula (see Figure 5-5, B). The concavity within the fossa is filled with the thick subscapularis muscle.
Proximal-To-Mid Humerus
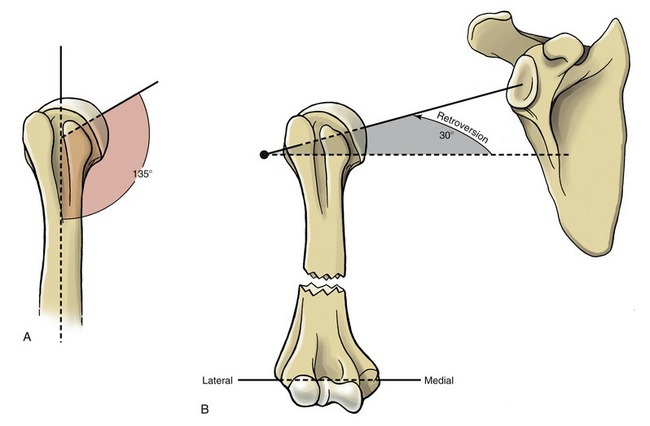
The head of the humerus, nearly one half of a full sphere, forms the convex component of the glenohumeral joint (Figure 5-7). The head faces medially and superiorly, forming an approximate 135-degree angle of inclination with the long axis of the humeral shaft (Figure 5-8, A). Relative to a medial-lateral axis through the elbow, the humeral head is rotated posteriorly about 30 degrees within the horizontal plane (see Figure 5-8, B). This rotation, known as retroversion (from the Latin retro, backward, + verto, to turn) aligns the humeral head within the scapular plane for articulation with the glenoid fossa (see Figure 5-4; angle C). Interestingly, researchers have shown that the dominant shoulder in elite baseball pitchers possesses greater humeral retroversion than the nondominant limb.24 This difference (which was not present in a control group of nonpitchers) was theorized to occur as an osseous adaptation to the large torsional stress generated during pitching.
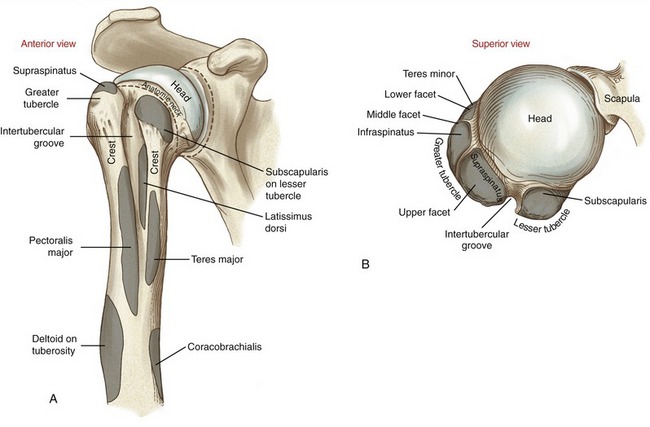
The anatomic neck of the humerus separates the smooth articular surface of the head from the proximal shaft (see Figure 5-7, A). The prominent lesser and greater tubercles surround the anterior and lateral circumference of the extreme proximal end of the humerus (see Figure 5-7, B). The lesser tubercle projects rather sharply and anteriorly for attachment of the subscapularis. The large and rounded greater tubercle has an upper, middle, and lower facet, marking the distal attachment of the supraspinatus, infraspinatus, and teres minor, respectively (see Figure 5-7, B and Figure 5-9).
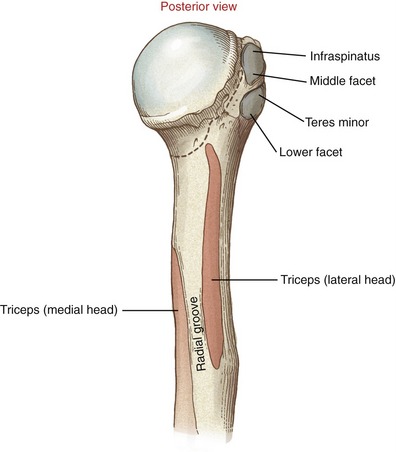
Sharp crests extend distally from the anterior side of the greater and lesser tubercles. These crests receive the distal attachments of the pectoralis major and teres major (see Figure 5-7, A). Between these crests is the intertubercular (bicipital) groove, which houses the tendon of the long head of the biceps brachii. The latissimus dorsi muscle attaches to the floor of the intertubercular groove, medial to the biceps tendon. Distal and lateral to the termination of the intertubercular groove is the deltoid tuberosity.
The radial (spiral) groove runs obliquely across the posterior surface of the humerus. The groove separates the proximal attachments of the lateral and medial head of the triceps (see Figure 5-9). Traveling distally, the radial nerve spirals around the posterior side of the humerus in the radial groove, heading toward the distal-lateral side of the humerus.
ARTHROLOGY
The most proximal articulation within the shoulder complex is the sternoclavicular joint (see Figure 5-1). The clavicle, through its attachment to the sternum, functions as a mechanical strut, or prop, holding the scapula at a relatively constant distance from the trunk. Located at the lateral end of the clavicle is the acromioclavicular joint. This joint, and associated ligaments, firmly attaches the scapula to the clavicle. The anterior surface of the scapula rests against the posterior-lateral surface of the thorax, forming the scapulothoracic joint. This articulation is not a true anatomic joint; rather, it is an interface between bones. Movements at the scapulothoracic joint are mechanically linked to the movements at both the sternoclavicular and acromioclavicular joints. The position of the scapula on the thorax provides a base of operation for the glenohumeral joint, the most distal and mobile link of the complex. The term “shoulder movement” describes the combined motions at both the glenohumeral and the scapulothoracic joints.
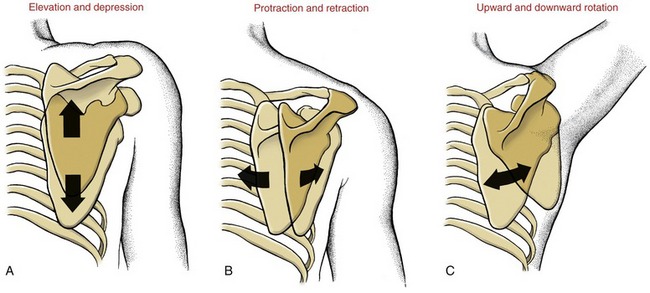
Before the kinematics of the sternoclavicular and acromioclavicular joints are described, the movements at the scapulothoracic joint must be defined (Figure 5-10). Primary movements at the scapulothoracic joint are traditionally described as elevation and depression, protraction and retraction, and upward and downward rotation. Additional movements of the scapula will be defined as the chapter unfolds.
Sternoclavicular Joint
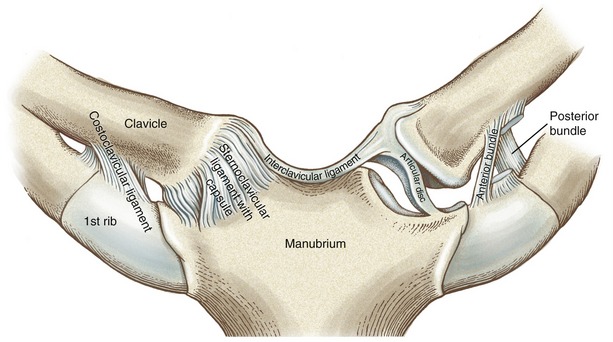
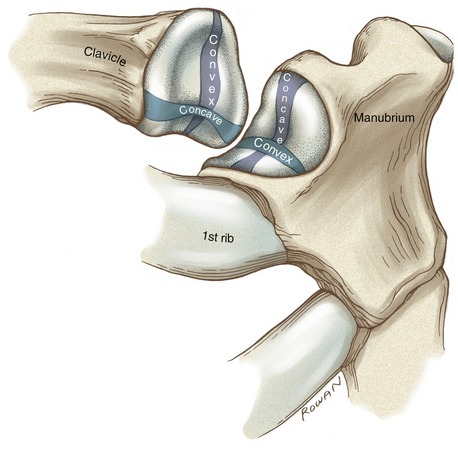
The sternoclavicular (SC) joint is a complex articulation, involving the medial end of the clavicle, the clavicular facet on the sternum, and the superior border of the cartilage of the first rib (Figure 5-11). The SC joint functions as the basilar joint of the entire upper extremity, linking the appendicular skeleton with the axial skeleton. The joint therefore must be firmly attached while simultaneously allowing considerable range of movement. These seemingly paradoxic functions are accomplished through extensive periarticular connective tissues, and an irregular saddle-shaped articular surface (Figure 5-12). Although highly variable, the medial end of the clavicle is usually convex along its longitudinal diameter and concave along its transverse diameter.178 The clavicular facet on the sternum typically is reciprocally shaped, with a slightly concave longitudinal diameter and a slightly convex transverse diameter.
PERIARTICULAR CONNECTIVE TISSUE
The SC joint is enclosed by a capsule reinforced by anterior and posterior sternoclavicular ligaments (see Figure 5-11).177 When active, muscles add further stability to the joint: anteriorly by the sternocleidomastoid, posteriorly by the sternothyroid and sternohyoid, and inferiorly by the subclavius. The interclavicular ligament spans the jugular notch, connecting the medial end of the right and left clavicles.
The costoclavicular ligament is a strong structure extending from the cartilage of the first rib to the costal tuberosity on the inferior surface of the clavicle. The ligament has two distinct fiber bundles running perpendicular to each other.178 The anterior bundle runs obliquely in a superior and lateral direction, and the posterior bundle runs obliquely in a superior and medial direction (see Figure 5-11). The crisscrossing of fibers assists with stabilizing the joint through all motions, except for a downward movement of the clavicle (i.e., depression).
The articular disc at the SC joint separates the joint into distinct medial and lateral joint cavities (see Figure 5-11).178 The disc is a flattened piece of fibrocartilage that attaches inferiorly near the lateral edge of the clavicular facet and superiorly at the sternal end of the clavicle and interclavicular ligament. The remaining outer edge of the disc attaches to the internal surface of the capsule. The disc not only strengthens the articulation but functions as a shock absorber by increasing the surface area of joint contact. This absorption mechanism apparently works well because significant age-related degenerative arthritis is relatively rare at this joint.35
The tremendous stability at the SC joint is due to the arrangement of the periarticular connective tissues and, to a lesser extent, the interlocking of the articular surfaces. Large forces through the clavicle often cause fracture of the bone before the SC joint dislocates. Clavicular fractures are most common in males under 30 years old—most often as the result of contact-sport or road-traffic accidents.164
KINEMATICS
The osteokinematics of the clavicle involve a rotation in all three degrees of freedom. Each degree of freedom is associated with one of the three cardinal planes of motion: sagittal, frontal, and horizontal. The clavicle elevates and depresses, protracts and retracts, and rotates around the bone’s longitudinal axis (Figure 5-13). The primary purpose of these movements is to place the scapula in an optimal position to accept the head of the humerus. Essentially all functional movements of the glenohumeral joint involve some movement of the clavicle around the SC joint. As described later in this chapter, the clavicle rotates in all three degrees of freedom as the arm is raised overhead.110,115,125,169
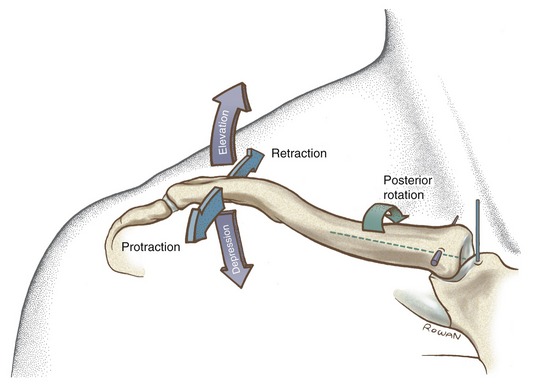
Elevation and Depression: Elevation and depression of the clavicle occur approximately parallel to the frontal plane, around a near anterior-posterior axis of rotation (see Figure 5-13). Maximums of approximately 45 degrees of elevation and 10 degrees of depression have been reported.27,140Elevation and depression of the clavicle produce a similar path of movement of the scapula.73
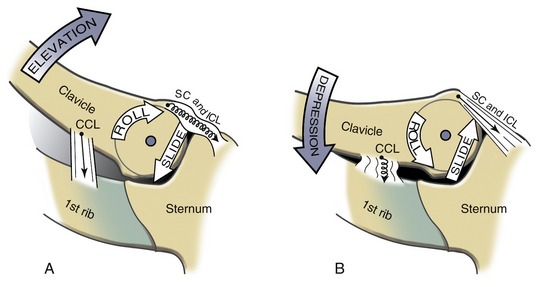
The arthrokinematics for elevation and depression of the clavicle occur along the SC joint’s longitudinal diameter (see Figure 5-12). Elevation of the clavicle occurs as its convex articular surface rolls superiorly and simultaneously slides inferiorly on the concavity of the sternum (Figure 5-14, A). The stretched costoclavicular ligament helps limit as well as stabilize the elevated position of the clavicle. Depression of the clavicle occurs by action of its convex surface rolling inferiorly and sliding superiorly (see Figure 5-14, B). A fully depressed clavicle elongates and stretches the interclavicular ligament and the superior portion of the capsular ligaments.
Protraction and Retraction: Protraction and retraction of the clavicle occur nearly parallel to the horizontal plane, around a vertical axis of rotation (see Figure 5-13). (The axis of rotation is shown in Figure 5-13 as intersecting the sternum because, by convention, the axis of rotation for a given motion intersects the convex member of the joint.) A maximum of 15 to 30 degrees of motion have been reported in each direction.27,140,179 The horizontal plane motions of the clavicle are strongly associated with protraction and retraction motions of the scapula.
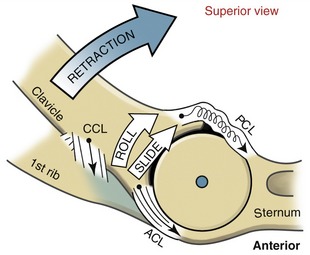
The arthrokinematics for protraction and retraction of the clavicle occur along the SC joint’s transverse diameter (see Figure 5-12). Retraction occurs as the concave articular surface of the clavicle rolls and slides posteriorly on the convex surface of the sternum (Figure 5-15). The end ranges of retraction elongate the anterior bundles of the costoclavicular ligament and the anterior capsular ligaments.
Axial (Longitudinal) Rotation of the Clavicle: The third degree of freedom at the SC joint is a rotation of the clavicle around the bone’s longitudinal axis (see Figure 5-13). During shoulder abduction or flexion, a point on the superior aspect of the clavicle rotates posteriorly 20 to 35 degrees.62,84,115,194 As the arm is returned to the side, the clavicle rotates back to its original position. The arthrokinematics of clavicular rotation involve a spin of its sternal end relative to the lateral surface of the articular disc.
Acromioclavicular Joint
The acromioclavicular (AC) joint is the articulation between the lateral end of the clavicle and the acromion of the scapula (Figure 5-16, A). The clavicular facet on the acromion faces medially and slightly superiorly, providing a point of attachment with the corresponding acromial facet on the clavicle. An articular disc of varying form is present in most AC joints.
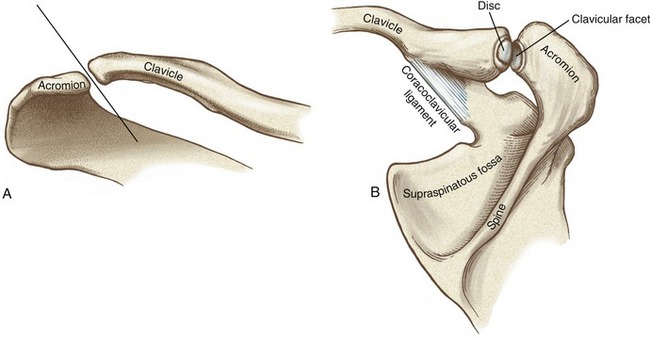
The AC joint is a gliding or plane joint, reflecting the predominantly flat contour of the joint surfaces. Joint surfaces vary, however, from flat to slightly convex or concave (see Figure 5-16, B). Because of the predominantly flat joint surfaces, roll-and-slide arthrokinematics are not described.
PERIARTICULAR CONNECTIVE TISSUE
The AC joint is surrounded by a capsule that is directly reinforced by superior and inferior ligaments (Figure 5-17).36,105 The superior capsular ligament is reinforced through attachments from the deltoid and trapezius.
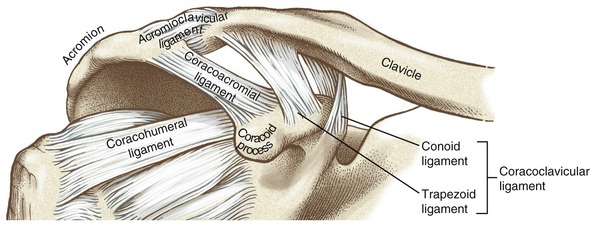
The coracoclavicular ligament provides an important extrinsic source of stability to the AC joint (see Figure 5-17). This extensive ligament consists of two parts: the trapezoid and conoid ligaments. The trapezoid ligament extends in a superior-lateral direction from the superior surface of the coracoid process to the trapezoid line on the clavicle. The conoid ligament extends almost vertically from the proximal base of the coracoid process to the conoid tubercle on the clavicle.
Both parts of the coracoclavicular ligament are of similar length, cross-sectional area, stiffness, and tensile strength.31 As a whole, the entire ligament is stronger and absorbs more energy at the point of rupture than most other ligaments of the shoulder. These structural features, in conjunction with the coracoclavicular ligament’s near-vertical orientation, suggest an important role in suspending the scapula (and upper extremity) from the clavicle.
The articular surfaces at the AC joint are lined with a layer of fibrocartilage and often separated by a complete or incomplete articular disc. An extensive dissection of 223 sets of AC joints revealed complete discs in only about 10% of the joints.35 The majority of joints possessed incomplete discs, which appeared fragmented and worn. According to DePalma,35 the incomplete discs are not structural anomalies but rather indications of the degeneration that often affects this joint.
Комментариев нет:
Отправить комментарий